
|
Plagio-What?
|
|
|||||||
 Roughly 1 baby out every 5, under the age of 6 months in the US, now suffers from plagiocephaly, meaning an abnormal head shape. Treatment for this condition is time consuming, expensive and often fraught with confusion for parents because of having to sort through conflicting information. The aim of this article is to present information on plagiocephaly so that parents have an easier time sorting through the process. It also offers tips on how to prevent plagiocephaly in section 7. |
||||||||
Plagiocephaly is an abnormal head shape in infants. Facial asymmetry, ear shifting and forehead sloping or bulging usually accompany it, although these features can be less noticeable. Plagiocephaly does not affect the brain. The 3 main types of plagiocephaly are: 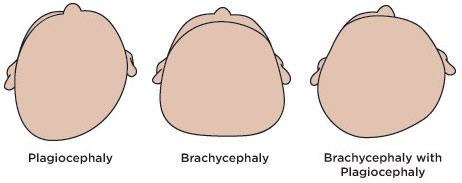
Plagiocephaly occurs when outside pressure is repeatedly applied to a particular area of the infant skull. Because infant skulls are soft and malleable, this pressure can alter their skull growth. This exterior pressure can also happen in utero, particularly with multiples or restricted space. Research finds that the average 2-month old baby now spends 15-16 hours a day on their back – allowing for a lot of external force to be placed on the same spot.
If parents notice their baby developing an unusual head shape they should bring it to the attention of their pediatrician. Pediatricians should also be assessing independently for this during routine visits. If there is reason for concern, pediatricians can refer parents to a cranio-facial specialist for further assessment or suggest/prescribe a helmet specialists on their own. To have a helmet made, usually a doctor must write a prescription for it.
This step can be confusing because when head abnormalities are mild to moderate, to treat a child or not, and how to treat a child, is largely a matter of opinion. Some pediatricians and specialists feel strongly about pursuing treatment, while others do not. Many waver someone in the middle. Those who do not pursue treatment may feel
During this step in the process parents should rely on what feels right to them. If an opinion is given which does not sit well with the parents, they should get additional opinions, research plagiocephaly on their own, visit a helmet provider independently for a consultation and/or ask to have their child’s head shape monitored. Ultimately the decision is up to the parents. A helpful question for parents to ask themselves during this process is, “if my baby’s head shape does not improve, will I feel comfortable with the type of treatment or lack of treatment I choose 10, 20 years from now?”
If you have decided to pursue treatment, the two main ways to do it are repositioning and helmeting your baby. Repositioning involves keeping your baby off of the misshapen part of their skull and making sure you alternate which part of their skull they are putting pressure on. Repositioning is not effective for asymmetrical deformities, so generally only brachycephaly deformities will respond to this type of treatment. Helmeting your baby is the typical form of treatment. The aim of the helmet is to encourage or allow skull growth in depressed areas while controlling the growth in prominent areas. Helmets are most effective between four to eighteen months of age, and are worn for a few weeks to a few months, depending on severity and age of the baby. Once parents have decided to move forward with getting a helmet for their baby, they must choose a helmet provider and the type of helmet, because not all helmets function the same although they may look similar. In fact, the most important aspect of helmet treatment providing a positive outcome is that the helmet is a good fit. The helmet should provide a snug, yet comfortable, hold on your baby’s more prominent areas while allowing space for growth in the depressed areas. Helmets that wiggle around do not provide the correct hold and straps should not be what keeps a helmet in place. The three major differences in helmet providers are:
In addition to parent’s choosing which helmet maker they feel will provide the best and most affective treatment, parents should also consider:
Many research studies have found that helmets do improve head shapes. However, the most recent study found virtually no difference in outcomes between baby’s that wore a helmet and those that did not at the age of 2. Researchers assigned 42 babies, age 5 and 6 months with mild to moderate plagiocephaly, to wear helmets for approximately 6 months. They had another 42 babies wear no helmets. When the children were 2 years old researchers were not able to distinguish between those who wore a helmet and those that did not. Only about a quarter of the babies in the study made a full recovery by age 2. Critics of the study say the study was inherently flawed due to treatment protocol, qualifications and experience of clinicians treating the infants, exclusion of infants with torticollis and severe head deformities and because the design, function and types of helmets used in the treatment were not regulated so even ill fitting helmets were included in the study. Parents should not use this latest study to influence their decision to helmet or not helmet their baby because of it's flaws, most notably the lack of oversight on the fit of the helmets used.
When plagiocephaly first begins it can be hard to spot. As the abnormality grows and your baby’s head grows, it can become more apparent. Ways to prevent plagiocephaly are:
|
||||||||
|
||||||||